Comments
No comments yet. You can be the first!
Most popular documents in this category





Content extract
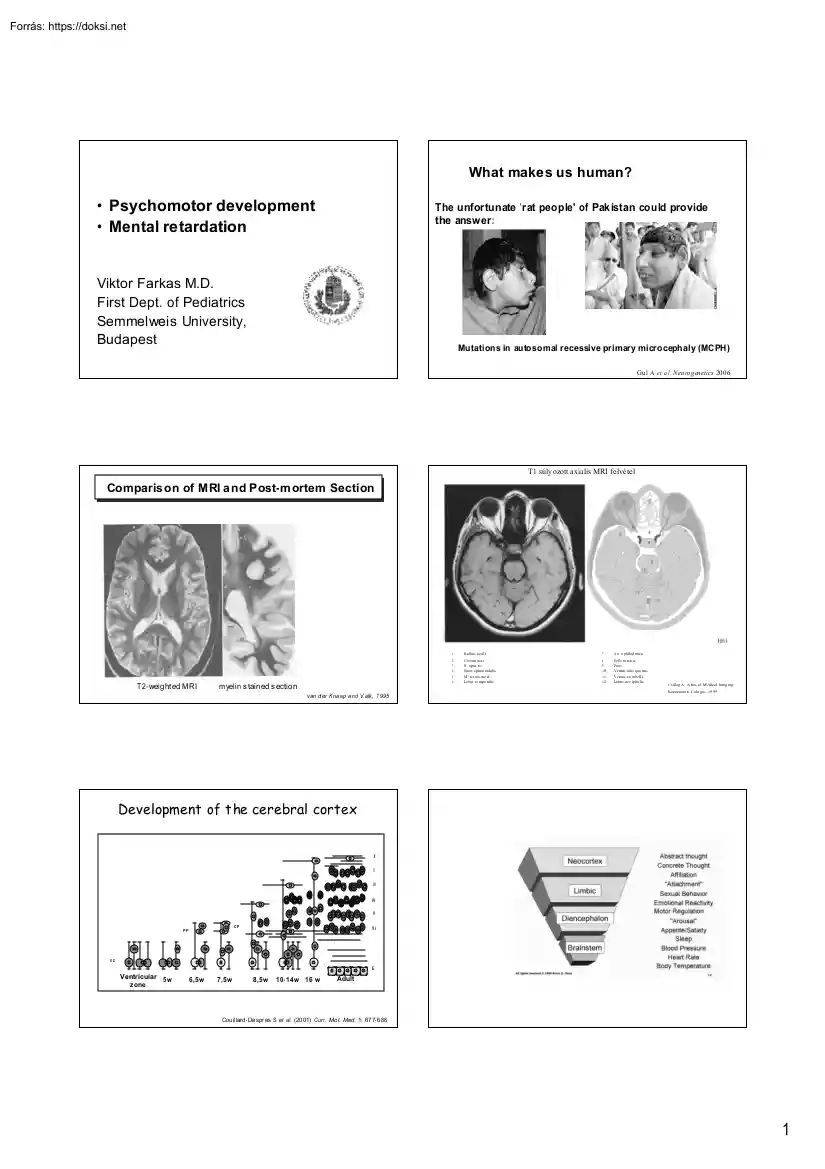
What makes us human? • Psychomotor development • Mental retardation The unfortunate 'rat people' of Pak istan could provide the answer: Viktor Farkas M.D First Dept. of Pediatrics Semmelweis University, Budapest Mutations in autosomal recessive primary microcephaly (MCPH) Gul A et a l. Neu ro g en etics 2006 T1 súly ozott axialis MRI felvé tel Comparis on of MRI a nd Post-m ortem Section T 2- weight ed MRI m yelin s tained s ection van d er Kna ap a nd V alk, 1 995 1. B ulbus ocul i 7. A rt. o phthal mica 2. 3. 4. 5. 6. C avum nas i N . optic us Sinus s phen oidalis M . rectus me d Lobus te mpo ralis 8. 9. 10. 11. 12. Se lla tu rcica Pons Ventric ulus qua rtus Vermis ce rebell i Lobus occ ipita lis Cs illag A, A tlas of M edical Imag ing, Koeneman n, Colo gne, 19 99 Development of t he cerebral cortex I II III IV V CP PP VI VZ E Ventricular 5w z one 6,5w 7,5w 8,5w 10- 14w 16 w Adult Cou il lard - De spr es S et al. (20 01) Curr Mo l Med 1:
67 7- 6 88 1 Development of the Human Brain Development of the Human Brain Development of Human Brain Development of Human Brain Myelinisation 2 Formation of the cerebral cortex Disorders of cortical development Shortly after the closure of the ro stral end of the neural tube: 1. Disorders of proliferation and differentiation of the neuronal progenitor cells 1. Proliferation of neuronal precursor cells and their differentiation into “ immature” neurons and glial cells 2. Disorders of migration 2 . Migration of post- mitotic immature neurons from the ventricular zone to the edge of the cerebral cortex 3. Disorders of cortical organisation (layering) 3 . Development of a mature cortex through the formation of cortical layers, synapse formation and apoptosis Migratory patterns of interneurons and pyramidal neurons converge in the dorsal cortex Development of t he cerebral cortex I II III IV V CP PP VI VZ E Ventricular 5w z one 6,5w 7,5w 8,5w 10- 14w 16
w Adult Cou il lard - De spr es S et al. (20 01) Curr Mo l Med 1: 67 7- 6 88 Ge nes involved in neuronal migration lissencephaly with cerebellar hypoplasia (LCHb) V LDLR simplified gyration with cerebellar hypoplasia P OM T1 Walker- Warburg- Synd rome (lissencephaly type II) P OM T2 Walker- Warburg- Synd rome (lissencephaly type II) P OM GnT1 Muscle- E ye- Brain Disease (lissencephaly type II ) Fukuti n Fukuyama Congenital Muscular Dystrophy (liss. type II) LIS I X - linked lissencepahly with abnormal genitalia (XLAG) Reelin BFPP X - linked isolated lissencephaly (lissencephaly type I ) ARX DCS DCX LIS I I isolated lissencepahly (lissencephaly type I ) PNH a.- r periventricular nodular heterotopia LIS 1 LCHb X - linked periventricular nodular heterotopia XLAG FLN A ARFGE F2 • subependymal / periventricular nod ular heterotopia (PNH) • lissencephal y t ype I (LI S I) / D ouble Cort ex Syndrome (DCS) FKRP congenital muscular dystrophy with
cerebellar cysts LARGE congenital muscular dystrophy with cortical malformation • lissencephal y with abnor mal genitalia (XLAG) GP R56 bilateral frontoparietal polymicrogyria • lissencephal y with cerebellar hypoplasia ( LCHb) • lissencephal y t ype II (LIS I I) • bilateral fr ont oparietal pol ymicrog yria (BFPP) 3 Periventricular Nodular Heterotopia (PNH) Periventricular Nodular Heterotopia (PNH) normal PNH • Cortex associated w ith epilepsy – up to 80% – freq. begin after age 20 – mostly focal seizures Cortex • cognitive impairment Heter otop ia Epen dym Epen dym • coagulopathy / vasculopathy ( stroke / patent ductus art. Botalli) • abortions A RFGEF2 gene autosomal- recessive F LN A gene X - linked microcephaly Periventricular Nodular Heterotopia (PNH) Mutations of F ilamin A g en e ( FL NA ), Xq28 Periventricular heterotopia: a disorder at the start of migration • Subsets of neur ons fail to migrate from the periventr
icular region during corticogenesis [XX ] mut - cause in heterozygous females PN H • PV NH due to mainly loss-offunction mutations in F LN A on Xq28 [X Y] mut - are in hemizygous male fetuses lethal • FLNA is an actin-binding protein Brain m alformations LIS I DCS PNH „Cobbles tone“ lissence phaly (lisse ncephaly type II) W alker-W arburg- Syndrom e M uscle- E ye- Brain- Disease BFPP LIS I I LCHb XLAG Fuku yam a congenit al muscular d ystrophy • subependymal / periventricular nod ular heterotopia (PNH) • lissencephal y t ype I (LI S I) / D ouble Cort ex Syndrome (DCS) - congenit al muscul ar dystrophy • lissencephal y with abnor mal genitalia (XLAG) - malf ormations of th e eyes • lissencephal y with cerebellar hypoplasia ( LCHb) • lissencephal y t ype II (LIS I I) • bilateral fr ont oparietal pol ymicrog yria (BFPP) - lissencephal y 4 „Cobbles tone“ lissence phaly (lisse ncephaly type II) „Cobbles tone“ lissence phaly
(lisse ncephaly type II) Fukuyama congenital muscular dystrophy Fukutin gene Sialinsäure Galaktose GlcNAc O-Mannose S ilan et al.(20 03), A n n Neur ol pachy gyria poly microgyria cerebellar hy poplasia cerebellar cysts eye abnormalities less prominent lif e expectancy 10- 20 y ears Ross (2002 ), Natu re A ida et al.(1 996), A JNR „Cobbles tone“ lissence phaly (lisse ncephaly type II) „Cobbles tone“ lissence phaly (lisse ncephaly type II) O - gly cosylation f ailure Ross (2002 ), Natu re Ross (2002 ), Natu re Autosomal recessive primary microcephaly Normal brain Patient with microc ephaly • Primary / true microcephaly is a subclass of microcephaly: - signif icant reductions in cerebral cortic al sizew ithout displaying other gross abnormalities • Affected individuals can have mild to moderate mental retardation and inf requently, epilepsy Autosomal recessive primary microcephaly (MCPH) Chromosome Gene MCPH1 Microcephaly + PVNH 8p22- pter Microcephalin
MCPH2 M icrocephaly 19q13.1- 1 32 MCPH3 Microcephaly 9q34 MCPH4 Microcephaly 15q15- q21 MCPH5 Microcephaly 1 q31 ASPM Microcephaly 13q12.2 CENPJ Microcephaly + PVNH 20q11 .21 ARFG EF2 MCHP6 - CDK5RAP2 - 5 Mutations in autosomal recessive primary microcephaly (MCPH) • Linkage study in 33 unrelated consanguinous Pakistani families – H ead circumferenc e 4 - 9 SD below population ag e- an d se x- related me an – Mild to moderat e mental ret ardation Tested 6 known MCPH loci Lin kag e: 18 f amilies linked to MCPH5 (ASPM gene) 2 f amilies linked to MCPH2 (chr. 19q) 2 f amilies to MCPH4 (chr. 15q) 1 famil y to MCPH6 (CENPJ gene) Mutations in ASPM f ound i n 9 of 18 families Mutations in regul ator y regions or anot her gene ? Gul A et a l . Neurogenetics 2006 Development of locomotion • Mothers are usually (but not always) right • Social, cultural and ethnic factors • Nor mal variations in development Development of locomotion Development of
locomotion • A, ventral suspension • B, prone position • C, sitting • D. standing and walking • E. manipulation (evolution of graps) • F. sphincter control Moro reflex: • Moro reflex • Parachute reaction • 6 Development of locomotion Ventral position: Abnormal newborn Ventral suspension A , normal B , pathological Abnormal newborn Development of locomotion Prone position Development of locomotion Sitting: normal newborn • Sitting 7 Primitive Reflexes – Stepping Primitive Reflexes - Stepping normal newborn • Primitiv e Reflexes - Stepping With the baby held in vertical suspension and his feet touching the mat, he does not have the expected reciprocal flexion and extension of th e legs . T he stepping o r walking reflex is absent in this baby. Development of locomotion Development of locomotion I: II: Standing and walking Development of locomotion • Manipulation (evolutaion of grasp) Standing and walking Head Circumference •
Another very important part of assessing brain development is measuring the grow th of the brain. This is accomplished by measuring the head circumference, w hic h is an accurate reflection of brain size . The brain grows to 80% of its adult volume during the first 2 years of lif e so many neurological diseases that occur early in lif e w ill impact the grow th of the brain. A small head (m icrocephaly) or a large head (macrocephaly or hydrocephalus) can be key findings in explaining the neurological abnormalities of a child. • It is essential to plot head circumference on a standardiz ed head grow th chart such as the Nellhaus chart. 8 SPECIAL PROGRAMS Neurodevelopment Assessment Head Circumference • Attentional based disorders • Dyslexia and language related learning difficulties • Study and organizational problems • Non-verbal learning disabilities • Emotional/Behavioral problems • Written Expression problems Developmental Milestones • The neurological
examination of the pediatric patient must be couched in the context of neurodevelopmental milestones. The normal neurological findings one w ould expect for a new born are certainly diff erent than a 2, 6 or 12-month-old infant. Obtaining developmental milestones is an important reflection of the maturation of the child’s nervous system and assessing development is an essential part of the pediatric neurological examination. De lay in obtaining developmental milestones and abnormal patterns of development are important indicators of underlying neurological disease. Cerebral Palsy Diseases - Therapies • • Speech Ther apy Occupational Therapy o r Phy sical Therap y • • • • • Vision Therap y Applied Behav ioral Anal ysis Therap y Neurodev elopment Therap y Specific Educatio nal Therap y ADD/ADHD • • • • • • • • • Autism ( als o PDD) Asperger Syndr ome Auditor y Processing D ysfu nctio n Dysgrap hia Dyslexia Men tal Retardati on Sensory Processing D
ys func tion Speech Disorders Vision Impaired • Th e R ita li n- Fr ee C hil d: M an a gi ng Hy per a ct ivi ty & A tt en ti on De fi cit s Wi t ho u t Dr u g s b y D ia na Hu n ter (ISBN 09 62 833 68 1 Risk factors for CP • multifactorial a persistent disorder of preterm birth multipl e gestation intraut erine growth r estriction male se x low Apg ar scores intraut erine infecti ons mat ernal thyroid abnor malities prena tal strokes - movement and - posture birth asph yxia mat ernal me th yl mercur y e xp osure mat ernal i odine deficienc y 9 Risk factors for CP Clinical course of CP CP generally is considered to be • prenatal factors result in 70-80% of cases of CP • In most cases: static encephalopathy or the e xact cause is unknown but is most likely multifactorial nonprogressive in nature !!!! Practice Parameter : Diagnostic Assessment of Practice Parameter : Diagnostic Assessment of the Child with Cerebra l Pa ls y (CP) the Child with Cerebra l
Pa ls y (CP) Neurology 2004; 62:851- 863 Neurology 2004; 62:851- 863 Prevalence • Worldw ide incidence of CP is approximately 2 to 2.5 per 1000 live births. • Each year about 10,000 babies born in the US develop CP. • Data from the Northern Ireland Cerebral Palsy Registry revealed that ½ the children w ith CP w ere of low birth w eight (i.e, less than 2500 grams Economic Impact: A California stud y (1992) of the e xtra e conomic costs associated with CP and 17 o ther congenital disorders (e.g, Down s yndrome, spina bifida) showed that CP had the highest lifetime costs per new case, a veraging $503,000 in 1992 dollars Rate of Cerebral Palsy • Rate of cere bral pals y per 1000 live births across Europe by year and se verity 10
67 7- 6 88 1 Development of the Human Brain Development of the Human Brain Development of Human Brain Development of Human Brain Myelinisation 2 Formation of the cerebral cortex Disorders of cortical development Shortly after the closure of the ro stral end of the neural tube: 1. Disorders of proliferation and differentiation of the neuronal progenitor cells 1. Proliferation of neuronal precursor cells and their differentiation into “ immature” neurons and glial cells 2. Disorders of migration 2 . Migration of post- mitotic immature neurons from the ventricular zone to the edge of the cerebral cortex 3. Disorders of cortical organisation (layering) 3 . Development of a mature cortex through the formation of cortical layers, synapse formation and apoptosis Migratory patterns of interneurons and pyramidal neurons converge in the dorsal cortex Development of t he cerebral cortex I II III IV V CP PP VI VZ E Ventricular 5w z one 6,5w 7,5w 8,5w 10- 14w 16
w Adult Cou il lard - De spr es S et al. (20 01) Curr Mo l Med 1: 67 7- 6 88 Ge nes involved in neuronal migration lissencephaly with cerebellar hypoplasia (LCHb) V LDLR simplified gyration with cerebellar hypoplasia P OM T1 Walker- Warburg- Synd rome (lissencephaly type II) P OM T2 Walker- Warburg- Synd rome (lissencephaly type II) P OM GnT1 Muscle- E ye- Brain Disease (lissencephaly type II ) Fukuti n Fukuyama Congenital Muscular Dystrophy (liss. type II) LIS I X - linked lissencepahly with abnormal genitalia (XLAG) Reelin BFPP X - linked isolated lissencephaly (lissencephaly type I ) ARX DCS DCX LIS I I isolated lissencepahly (lissencephaly type I ) PNH a.- r periventricular nodular heterotopia LIS 1 LCHb X - linked periventricular nodular heterotopia XLAG FLN A ARFGE F2 • subependymal / periventricular nod ular heterotopia (PNH) • lissencephal y t ype I (LI S I) / D ouble Cort ex Syndrome (DCS) FKRP congenital muscular dystrophy with
cerebellar cysts LARGE congenital muscular dystrophy with cortical malformation • lissencephal y with abnor mal genitalia (XLAG) GP R56 bilateral frontoparietal polymicrogyria • lissencephal y with cerebellar hypoplasia ( LCHb) • lissencephal y t ype II (LIS I I) • bilateral fr ont oparietal pol ymicrog yria (BFPP) 3 Periventricular Nodular Heterotopia (PNH) Periventricular Nodular Heterotopia (PNH) normal PNH • Cortex associated w ith epilepsy – up to 80% – freq. begin after age 20 – mostly focal seizures Cortex • cognitive impairment Heter otop ia Epen dym Epen dym • coagulopathy / vasculopathy ( stroke / patent ductus art. Botalli) • abortions A RFGEF2 gene autosomal- recessive F LN A gene X - linked microcephaly Periventricular Nodular Heterotopia (PNH) Mutations of F ilamin A g en e ( FL NA ), Xq28 Periventricular heterotopia: a disorder at the start of migration • Subsets of neur ons fail to migrate from the periventr
icular region during corticogenesis [XX ] mut - cause in heterozygous females PN H • PV NH due to mainly loss-offunction mutations in F LN A on Xq28 [X Y] mut - are in hemizygous male fetuses lethal • FLNA is an actin-binding protein Brain m alformations LIS I DCS PNH „Cobbles tone“ lissence phaly (lisse ncephaly type II) W alker-W arburg- Syndrom e M uscle- E ye- Brain- Disease BFPP LIS I I LCHb XLAG Fuku yam a congenit al muscular d ystrophy • subependymal / periventricular nod ular heterotopia (PNH) • lissencephal y t ype I (LI S I) / D ouble Cort ex Syndrome (DCS) - congenit al muscul ar dystrophy • lissencephal y with abnor mal genitalia (XLAG) - malf ormations of th e eyes • lissencephal y with cerebellar hypoplasia ( LCHb) • lissencephal y t ype II (LIS I I) • bilateral fr ont oparietal pol ymicrog yria (BFPP) - lissencephal y 4 „Cobbles tone“ lissence phaly (lisse ncephaly type II) „Cobbles tone“ lissence phaly
(lisse ncephaly type II) Fukuyama congenital muscular dystrophy Fukutin gene Sialinsäure Galaktose GlcNAc O-Mannose S ilan et al.(20 03), A n n Neur ol pachy gyria poly microgyria cerebellar hy poplasia cerebellar cysts eye abnormalities less prominent lif e expectancy 10- 20 y ears Ross (2002 ), Natu re A ida et al.(1 996), A JNR „Cobbles tone“ lissence phaly (lisse ncephaly type II) „Cobbles tone“ lissence phaly (lisse ncephaly type II) O - gly cosylation f ailure Ross (2002 ), Natu re Ross (2002 ), Natu re Autosomal recessive primary microcephaly Normal brain Patient with microc ephaly • Primary / true microcephaly is a subclass of microcephaly: - signif icant reductions in cerebral cortic al sizew ithout displaying other gross abnormalities • Affected individuals can have mild to moderate mental retardation and inf requently, epilepsy Autosomal recessive primary microcephaly (MCPH) Chromosome Gene MCPH1 Microcephaly + PVNH 8p22- pter Microcephalin
MCPH2 M icrocephaly 19q13.1- 1 32 MCPH3 Microcephaly 9q34 MCPH4 Microcephaly 15q15- q21 MCPH5 Microcephaly 1 q31 ASPM Microcephaly 13q12.2 CENPJ Microcephaly + PVNH 20q11 .21 ARFG EF2 MCHP6 - CDK5RAP2 - 5 Mutations in autosomal recessive primary microcephaly (MCPH) • Linkage study in 33 unrelated consanguinous Pakistani families – H ead circumferenc e 4 - 9 SD below population ag e- an d se x- related me an – Mild to moderat e mental ret ardation Tested 6 known MCPH loci Lin kag e: 18 f amilies linked to MCPH5 (ASPM gene) 2 f amilies linked to MCPH2 (chr. 19q) 2 f amilies to MCPH4 (chr. 15q) 1 famil y to MCPH6 (CENPJ gene) Mutations in ASPM f ound i n 9 of 18 families Mutations in regul ator y regions or anot her gene ? Gul A et a l . Neurogenetics 2006 Development of locomotion • Mothers are usually (but not always) right • Social, cultural and ethnic factors • Nor mal variations in development Development of locomotion Development of
locomotion • A, ventral suspension • B, prone position • C, sitting • D. standing and walking • E. manipulation (evolution of graps) • F. sphincter control Moro reflex: • Moro reflex • Parachute reaction • 6 Development of locomotion Ventral position: Abnormal newborn Ventral suspension A , normal B , pathological Abnormal newborn Development of locomotion Prone position Development of locomotion Sitting: normal newborn • Sitting 7 Primitive Reflexes – Stepping Primitive Reflexes - Stepping normal newborn • Primitiv e Reflexes - Stepping With the baby held in vertical suspension and his feet touching the mat, he does not have the expected reciprocal flexion and extension of th e legs . T he stepping o r walking reflex is absent in this baby. Development of locomotion Development of locomotion I: II: Standing and walking Development of locomotion • Manipulation (evolutaion of grasp) Standing and walking Head Circumference •
Another very important part of assessing brain development is measuring the grow th of the brain. This is accomplished by measuring the head circumference, w hic h is an accurate reflection of brain size . The brain grows to 80% of its adult volume during the first 2 years of lif e so many neurological diseases that occur early in lif e w ill impact the grow th of the brain. A small head (m icrocephaly) or a large head (macrocephaly or hydrocephalus) can be key findings in explaining the neurological abnormalities of a child. • It is essential to plot head circumference on a standardiz ed head grow th chart such as the Nellhaus chart. 8 SPECIAL PROGRAMS Neurodevelopment Assessment Head Circumference • Attentional based disorders • Dyslexia and language related learning difficulties • Study and organizational problems • Non-verbal learning disabilities • Emotional/Behavioral problems • Written Expression problems Developmental Milestones • The neurological
examination of the pediatric patient must be couched in the context of neurodevelopmental milestones. The normal neurological findings one w ould expect for a new born are certainly diff erent than a 2, 6 or 12-month-old infant. Obtaining developmental milestones is an important reflection of the maturation of the child’s nervous system and assessing development is an essential part of the pediatric neurological examination. De lay in obtaining developmental milestones and abnormal patterns of development are important indicators of underlying neurological disease. Cerebral Palsy Diseases - Therapies • • Speech Ther apy Occupational Therapy o r Phy sical Therap y • • • • • Vision Therap y Applied Behav ioral Anal ysis Therap y Neurodev elopment Therap y Specific Educatio nal Therap y ADD/ADHD • • • • • • • • • Autism ( als o PDD) Asperger Syndr ome Auditor y Processing D ysfu nctio n Dysgrap hia Dyslexia Men tal Retardati on Sensory Processing D
ys func tion Speech Disorders Vision Impaired • Th e R ita li n- Fr ee C hil d: M an a gi ng Hy per a ct ivi ty & A tt en ti on De fi cit s Wi t ho u t Dr u g s b y D ia na Hu n ter (ISBN 09 62 833 68 1 Risk factors for CP • multifactorial a persistent disorder of preterm birth multipl e gestation intraut erine growth r estriction male se x low Apg ar scores intraut erine infecti ons mat ernal thyroid abnor malities prena tal strokes - movement and - posture birth asph yxia mat ernal me th yl mercur y e xp osure mat ernal i odine deficienc y 9 Risk factors for CP Clinical course of CP CP generally is considered to be • prenatal factors result in 70-80% of cases of CP • In most cases: static encephalopathy or the e xact cause is unknown but is most likely multifactorial nonprogressive in nature !!!! Practice Parameter : Diagnostic Assessment of Practice Parameter : Diagnostic Assessment of the Child with Cerebra l Pa ls y (CP) the Child with Cerebra l
Pa ls y (CP) Neurology 2004; 62:851- 863 Neurology 2004; 62:851- 863 Prevalence • Worldw ide incidence of CP is approximately 2 to 2.5 per 1000 live births. • Each year about 10,000 babies born in the US develop CP. • Data from the Northern Ireland Cerebral Palsy Registry revealed that ½ the children w ith CP w ere of low birth w eight (i.e, less than 2500 grams Economic Impact: A California stud y (1992) of the e xtra e conomic costs associated with CP and 17 o ther congenital disorders (e.g, Down s yndrome, spina bifida) showed that CP had the highest lifetime costs per new case, a veraging $503,000 in 1992 dollars Rate of Cerebral Palsy • Rate of cere bral pals y per 1000 live births across Europe by year and se verity 10
 When reading, most of us just let a story wash over us, getting lost in the world of the book rather than paying attention to the individual elements of the plot or writing. However, in English class, our teachers ask us to look at the mechanics of the writing.
When reading, most of us just let a story wash over us, getting lost in the world of the book rather than paying attention to the individual elements of the plot or writing. However, in English class, our teachers ask us to look at the mechanics of the writing.